
What is Premature Ejaculation?
Premature ejaculation (PE) is when a man has a tendency to ejaculate quickly after penetration, without the feeling of control, and where it causes distress to him and/or his partner. Although it's hard to define PE by standard medical metrics, in our opinion, you know when you have it. In other words, if you feel you have PE, so do we.
PE is considered the most common sexual dysfunction in men, with studies finding that 20-30% of men suffer from PE 16. At Maze, we will determine the cause of your PE and customize the best treatment plan for you.
What is PE?
Treatment Options for PE
Psychological Causes of PE
Helpful Resources
Two Types of PE
The formal definition of PE by the International Society for Sexual Medicine (ISSM) is probably the most useful and widely accepted to date. Importantly, it divides PE into two categories:
- Lifelong-Premature Ejaculation (LL-PE): affects men from the time they first become sexually active and is primarily physical, and not psychological, in origin. It can always be managed successfully if a man is motivated and if he realizes that Lifelong PE will require lifelong active management.
- Acquired Premature Ejaculation (A-PE): develops later in life after having normal ejaculatory control at one time. It can often be cured but even when it cannot be cured, it can be managed quite successfully, usually with a combination of behavioral and medical modalities.
Interestingly, the origin of the PE and thus the treatment may be quite different for these two groups.
Definitions of PE Explained
Currently all medical definitions of premature ejaculation involve intercourse involving a vagina. Clearly the same definition will apply to both gay or straight men who ejaculate prematurely while having anal sex. In fact, since the average anus is tighter than the average vagina, ejaculation may occur even more quickly during anal intercourse.
The ISSM definition of premature ejaculation is that of a male sexual dysfunction characterized by:
- Ejaculation that always or nearly always occurs prior to or within about 1 minute of vaginal penetration from the first sexual experience (lifelong PE) or,
- A clinically significant and bothersome reduction in latency time, often to about three minutes or less (acquired PE)
- The inability to delay ejaculation on all or nearly all vaginal penetrations
- Causes negative personal consequences, such as distress, bother, frustration, and/or avoidance of sexual intimacy.
This definition has many problems. The first issue is why 60 seconds was chosen as the cut-off for PE.
It is based on a population study which tried to quantify how long intercourse actually took for the “average” couple. The time from when a man inserts his penis into his partner’s vagina until he ejaculates is called the “intravaginal latency time” (IELT). In this study, average IELT was 5.4 minutes, or 5 minutes and 24 seconds. Then, like statisticians like to do, they calculated out that 97.5% of men have an IELT of greater than 60 seconds. The 2.5% who ejaculate in less than 60 seconds are thus two standard deviations below the mean, and thus are considered outside the norm.
However, for the vast majority of men (and their partners), an IELT of slightly more than 60 seconds would not lead to satisfactory intercourse. This definition, though scientific, is inherently flawed and thus we have always chosen to use a more liberal definition:
“Premature Ejaculation is when a man has a tendency to ejaculate quickly after penetration, without the feeling of control, and where it causes distress to him and or his partner.”
Occasionally, men have an unrealistic view of how long they are supposed to last. His partner may take 30 minutes to reach a climax, and thus the man feels he has PE if he doesn’t last that long. Or, from watching videos, he imagines that men are supposed to last for as long as they want, change positions frequently, never losing their erection, and then ejaculate with total control after or exactly while their partner is achieving her/his orgasm. These men do not have PE, but that doesn’t mean we can’t help them to achieve their goals.
PE Treatment Options
It is important to remember that men with lifelong premature ejaculation (LL-PE), are “just built this way.” Thus, it is more accurate to say that LL-PE is managed rather than cured.
Men with acquired premature ejaculation (A-PE) can be cured of PE when the reason they developed PE is treated. Also, men with A-PE, when managed similarly to men with LL-PE, may have a resolution of their PE.
The treatment options can be divided into behavioral and pharmacologic (medications). The medications can be divided into systemic therapies (pills) and local/topical therapies (creams or sprays).
We find that our patients do the best when they use multiple modalities to manage their PE. In other words, when they combine behavioral and medical modalities, they last longer.
Behavioral Treatments for PE
Behavioral Treatments may be quite useful for many men in managing their PE. Behavioral techniques include:
The “start/stop” and the “squeeze” techniques
Behavioral treatments for PE were traditionally ways to slow men down from ejaculating during intercourse. These included the “start-stop” technique and the “squeeze” techniques. These have been conclusively been shown not to be curative, and they clearly interfere with the enjoyment of intercourse. In general, we have not recommended these or used them in our therapies.
Increasing Ejaculatory Threshold Through Recent Ejaculation
After you ejaculate, you are less excited/excitable than prior to ejaculating. All men will ejaculate more quickly from intercourse if they have not ejaculated for a long time — the longer it has been since you ejaculated, the faster you will have a tendency to ejaculate. We can take advantage of this, by diminishing your physiological excitement, by having you ejaculate prior to intercourse or (depending on age) at the very beginning of love making.
Masturbation Prior to Intercourse
You will need to figure out how long after ejaculation it takes you to be able to get an erection again. This is called the refractory period. (This time can be diminished by taking a PDE5 inhibitor, like Viagra, Levitra, Cialis, or Stendra, prior to intercourse.) Ideally, you would then masturbate this amount of time prior to intercourse, or as close to this as possible. Thus, if your refractory period is two hours, you would aim to masturbate two hours prior to intercourse.
Regarding masturbation, we also sometimes recommend using masturbation sleeves to help desensitize the penis.
Sandwich Technique
Some men, particularly younger men, have a very short refractory period. This means they can get another erection very quickly after ejaculation. This ability can be taken advantage of by using the “Sandwich Technique.” In this technique, a sexual session begins with having the man with PE ejaculate first, either through oral, manual, anal or vaginal stimulation, but without a lot of foreplay. Then the man who has just recently ejaculated turns the attention to his partner, getting her/him very excited. His partner’s excitement will get the man with PE excited, and he will then get erect and penetrate, and be able to last longer than the first time. This can be a very satisfying model, as the man gets two orgasms (which of course makes both him and his partner happy) and he lasts longer prior to the second orgasm.
Sexual Positions
There is a lot of debate on this topic, but most agree that the missionary position and “coming in from behind”, are probably two of the worst positions for men with PE. Partner on top and man sitting seem to be better. One of the theories is that if the man does not need to do active thrusting he may last longer. It is important that you experiment yourself with what works for you.
Medical Treatments for PE
Medical treatments for PE can be broken down into topical agents (applied to the skin of the penis) and oral medications, taken by mouth.
Topical Treatments for PE
Numbing agents can be used to delay ejaculation. It makes sense that if the penis is less sensitive, it will take more stimulation in order to trigger ejaculation. Many men have found this successful. The two medications we use the most are EMLA cream and Promescent.
Many men will last longer after penetration. However, many men do not like this modality. They do not like the feeling of their penis being numb, even if it leads to a longer thrusting time. Some men will have difficulty getting and/or maintaining their erection, because of the numbness. Some partners may be sensitive to the taste and or smell, even after it has been wiped off.
EMLA Cream:
EMLA Cream is an equal combination of lidocaine 2.5% and prilocaine 2.5%. It is available by prescription only. It can also be written as a generic, which may save money. It is a topical anesthetic, which can be used off-label for PE.
You place the EMLA Cream on your penis 15-20 minutes before you plan to have sex. You can cover the head of the penis, or the shaft, or both. Prior to intercourse, you should wipe it off, so that your partner’s mouth, vagina, or anus does not get numb. The anesthetic effects will remain.
Promescent
Promescent is a topical anesthetic spray specifically for men with PE. It comes in a discreet pocket size. Men usually start with three sprays on the most sensitive area of the penis, which is the frenulum (the back of the tip). The spray is then rubbed in. After 10-20 minutes, the maximal numbing should have occurred, and the medication can be wiped off. Some men use up to 10 sprays. Since it is over the counter, you can order it directly on-line from the company at www.promescent.com.
Oral Medications for PE
The ideal medical treatment for PE would be a pill taken right before intercourse, which delays ejaculation with no side effects, and then is out of your system almost immediately. This, unfortunately, does not exist yet, but is an area of active research. Many medications have been tried and are being used for PE. In Europe, and much of the world, dapoxetine, a short acting serotonin selective reuptake inhibitor (SSRI) has been approved and is used for PE. It has not been approved for use in the US. The most commonly prescribed class of medications for PE in the US are the SSRI’s.
Dapoxetine
Dapoxetine is a short acting SSRI, available in Europe and many other countries (including Mexico). It is marketed under the brand names of Priligy and Westoxetin. It is ideally taken 1-3 hours before intercourse. It was not approved by the FDA, and thus is not available in the United States.
Other Serotonin Selective Reuptake Inhibitors (SSRI’s)
SSRIs are prescribed extremely frequently for depression, anxiety, obsessive compulsive disorder, and irritability. However, they are known to have two major sexual side effects in many men and women — they may make it harder to reach a climax, and they may decrease libido.
The side effect of delaying climax can be used as a treatment for men with premature ejaculation.
However, these medications are not FDA approved for the treatment of PE. This does not mean they cannot be used, “off-label.” Indeed, they are, in our experience, the most effective single treatment for PE.
SSRI’s are all very long-acting, meaning they take a while to reach good levels after you start them, and they stay in your system for a long time. It makes sense that a medication to treat depression would be designed to stay in your system for a long time, with relatively constant levels throughout the day. Otherwise, someone undergoing treatment might have frequent mood fluctuations.
The fact that they are long acting, means it takes a long time to get good levels in your system, and thus it is difficult to use them on an as needed basis, just prior to intercourse. Some men are exquisitely sensitive to the SSRI’s and can use them on an as needed basis, but this is very unusual.
Thus, in order for them to be effective, most men need to be on them long term.
Many men are worried about the long term side effects of the SSRI’s. We have found that most men have minimal side effects, and very good efficacy. Many men with low grade depressions, notice an improvement in their moods. Many men also notice a decrease in their anxiety levels, less irritability, and less obsessiveness. Men without depression, irritability, or anxiety almost never notice any mood changes.
Which SSRI’s are Used for PE?
The three SSRI’s with the most effect on ejaculation are paroxetine (Paxil), sertraline (Zoloft), and fluoxetine (Prozac.) All three are available as generics.
We usually use sertraline, as it easy to dose and seems to have few side effects.
The maximum dosage is 200mg, and many men need this amount.
We always start at 25mg, and then go up by 25 mg weekly, biweekly, or monthly. Many men are very anxious to be managed as quickly as possible, and are less concerned with temporary side effects. These men have their dosages increased rapidly. Other men are more concerned about temporary side effects and less concerned about responding so quickly. For these men, we increase the dosage slowly.
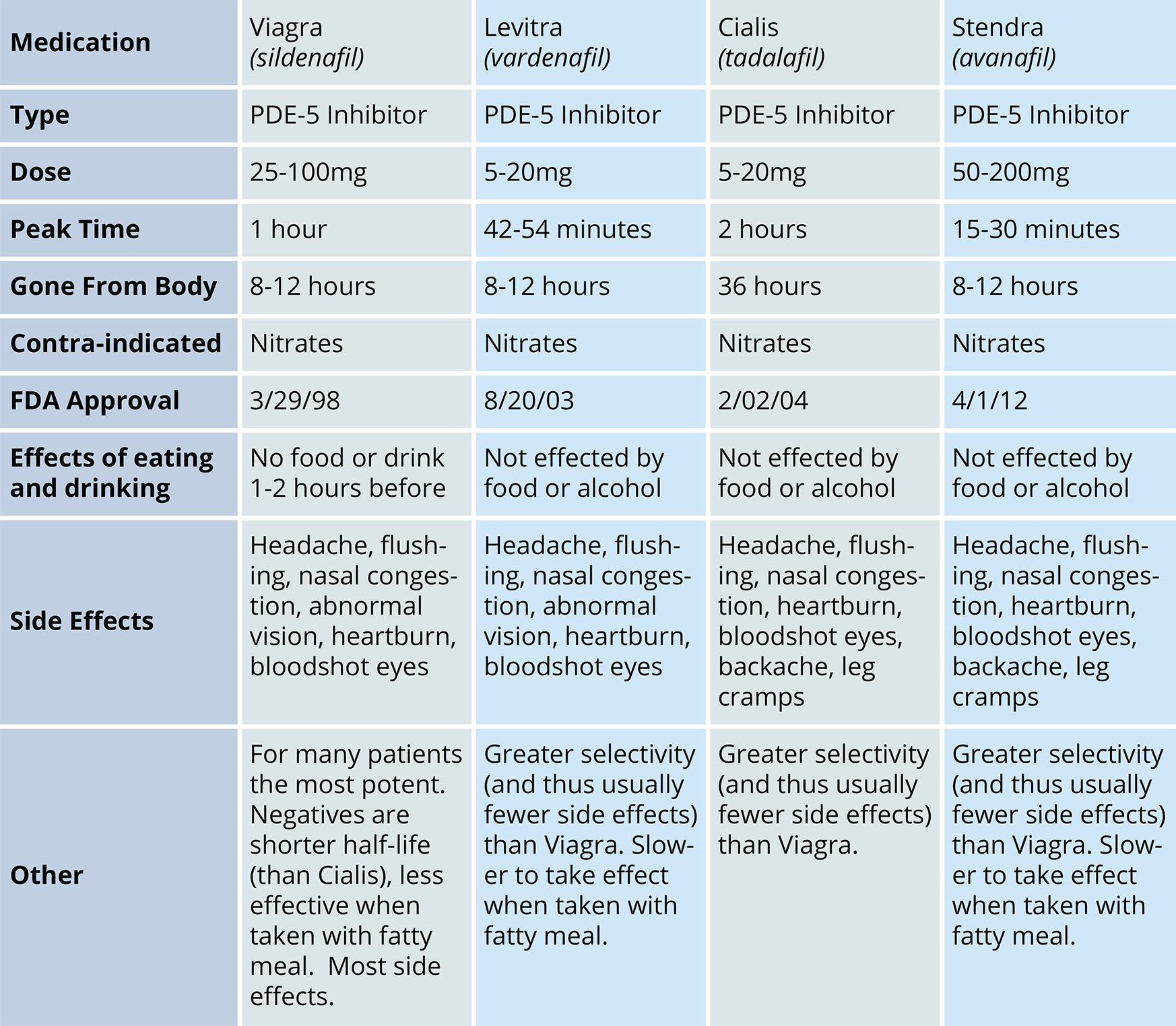
PDE5 Inhibitors (Viagra, Levitra, Cialis, Stendra) for Premature Ejaculation
The PDE5 inhibitors (PDE5’s) do not delay ejaculation. However, they may be useful in the management of premature ejaculation. They may make it easier for a man to:
- Get and maintain an erection, even if a topical anesthetic (numbing cream) is used. Also, since many men with erectile dysfunction develop PE, better erections more easily maintained can reverse the developed PE.
- Get a second erection sooner after having ejaculated (whether prior to sexual relations or during sexual relations.)
- Maintain an erection through ejaculation, and continue thrusting.
If possible the specific PDE5 would be at its peak efficacy when you went to have intercourse. Thus, Viagra and Levitra should be taken one hour prior to intercourse, Cialis two hours prior, and Stendra 30 minutes prior.
Intracavernosal Injections for PE
Intracavernosal injections are one of the most effective ways of treating erectile dysfunction. They can get most men superb erections, which are rigid and easy to maintain. They can be used in men with PE to get a man erections that stay rigid even after climaxing, so the man can continue thrusting and satisfy his partner. Many of these men will even have a second orgasm without losing the erection.
In our minds, this is a vastly underused technique for management of PE.
Combination Treatments for PE
Many men will need only one of the modalities described above. For example, their PE is completely managed by a single SSRI, or topical medications, or behavioral techniques alone. However for some men, a single modality does not get them to last long enough. Thus to optimally manage their PE, these men will use a combination of the above techniques.
Sample Schedule
For a man with a refractory period (time between erections) of two hours, planning to have intercourse at 9PM, the schedule might be:
7:00 PM — Masturbate and take Cialis 5-20mg
8:40 PM — Apply a topical anesthetic
9:00 PM — Begin relations. During relations, depending on the age and refractory period of the man, the sandwich technique can be used.
Many men and/or their partners are unwilling to plan intercourse, feeling that the lack of spontaneity detracts too significantly from the pleasure. For these men, the SSRI’s are the best option. For many men and/or their partners planned long lasting sex is better than unplanned short or shorter lasting sex, and they and their partners will use some kind of combination therapy, if single modality therapy is inadequate.
What exactly is ejaculation?
It is important to remember that the culmination of intercourse actually consists of three separate but linked events.
Emission
The first step is emission. This is the depositing of the ejaculate (seminal fluid) in the urethra (which is the tube you urinate and ejaculate from.) The fluid in the urethra then triggers the next step, ejaculation.
Ejaculation
Ejaculation is the rhythmic contraction of the muscles surrounding the urethra, which forces the fluid out.
Orgasm
Orgasm is a pleasurable altered state of consciousness that usually corresponds to the time of emission and ejaculation.
Thus premature ejaculation can really be viewed as initiating this whole climactic process earlier than a man and/or his partner would like. However, once emission occurs, orgasm and ejaculation normally follow.
What factors affect ejaculation?
It is important to understand what factors affect ejaculation, in order to understand what evaluation needs to be done. Correctly identifying a particular man’s reasons for having premature ejaculation helps us treat him most effectively.
Ejaculation is Affected By
- The Central Nervous System (your brain and spinal cord)
- Hormones
- Prostate
- Sexual Function/Erectile Dysfunction
Central Nervous System
The signals directing your brain and spinal cord are chemicals called “neurotransmitters.” All of these neurotransmitters can affect ejaculation. However, the two thought to have the most effect on ejaculation are serotonin and dopamine.
Serotonin
Evidence suggests that Serotonin is the main neurotransmitter regulating ejaculation and that Serotonin’s effect is to delay ejaculation. This is the reason why the class of drugs called the Serotonin Selective Reuptake Inhibitors (SSRI’s) can help delay ejaculation. In fact, virtually any drug that increases serotonin delays ejaculation.
Dopamine
Dopamine, the second most important neurotransmitter regulating ejaculation, seems to have the opposite effect. Increasing dopamine has a promoting effect on ejaculation, making it occur with a lower threshold and thus more quickly. Drugs that increase dopamine have been used to make it easier for men with delayed ejaculation to reach a climax.
Separately, any chemicals that affect the nerves outside the brain and spinal cord (i.e. the peripheral nervous system) can also affect ejaculation. The two chemicals that seem to affect the nerves are oxytocin and vasopressin. However, the nature and importance of their role in ejaculation is still unknown.
Hormones
Thyroid Hormone
Increased thyroid hormone (hyperthyroidism) can cause and/or contribute to premature ejaculation. Thus, testing thyroid hormone levels is an important part of a PE evaluation.
Correcting hyperthyroidism can increase a man’s ejaculatory control and IELT (Intravaginal Ejaculatory Latency Time).
Men with decreased thyroid hormone may have a harder time reaching climax.
Testosterone
Testosterone clearly is the central hormone in male sexual function. Low testosterone levels can lead to a decreased libido, and erectile dysfunction. Erectile dysfunction is a common contributor to premature ejaculation, especially acquired premature ejaculation. It is important to check testosterone levels, as well as evaluate a man’s erectile function while doing a PE evaluation.
Prostate
The prostate is clearly involved in ejaculation. Its function is to produce a clear fluid that makes up about one third of the ejaculate. The nerves running in the area of the prostate are responsible for ejaculation. Many men are capable of reaching climax exclusively from prostatic stimulation. Some spinal cord injured men can be made to ejaculate through intense electric stimulation of these nerves (electroejaculation).
Men with prostatitis have been found to have a higher incidence of premature ejaculation, especially acquired ejaculation. When men with prostatitis are treated, almost two thirds of them will have an improvement in their PE (increased IELT). Thus it is very important that a prostate exam be part of any evaluation for acquired PE.
Erectile Dysfunction
There is a complicated relationship but definite correlation between erectile dysfunction and premature ejaculation. Many men with long standing PE, particularly lifelong PE, will begin losing their confidence sexually. This may cause erection issues.
Men with erection issues develop PE quite often. There are several theories as to why this happen. It may be that a man pushes himself to be excited and/or ejaculate earlier because he is afraid of losing his erection. It is possible that his increased anxiety levels from his erection issues can trigger early ejaculation.
It is crucial that the sexual/erectile function of all men with PE be assessed thoroughly.
Genetics
Since premature ejaculation seems to run in families and has a physical basis, it makes sense that there would be a genetic component to it. This area of research is just beginning, but it seems like there may be abnormality of the serotonin receptor.
Visiting a Doctor — Understanding the Underlying Problem
A first appointment will typically be between 45 and 60 minutes. It will include both a verbal history and a physical exam. We will take a thorough medical history in order to place your premature ejaculation in the context of your history. This may include questions such as how long you last prior to ejaculation. Some men ejaculate during foreplay. There are men who even ejaculate while in the process of getting undressed and before significant contact has occurred. Others penetrate, but ejaculate much earlier than they would like and spend most of the time inside attempting not to ejaculate.
Some other questions include:
- What is the quality of your erections?
- What happens when you try to have intercourse?
- Do you have decreased rigidity?
- Do you have difficulty maintaining your erection?
- At what point do you lose your erection?
- Do you wake up in the morning or at any point while sleeping with an erection?
- How rigid are the nocturnal erections?
- What is your sexual interest level (libido) like?
- Does your penis have a curve, bend, or twist in it when it is rigid?
- What is the status of your relationship? Are you married, divorced, single, gay, etc.?
- How is the relationship going?
You might have an issue of premature ejaculation along with erectile dysfunction. Here, it’s very important to determine which came first. Many men with erectile dysfunction have difficulty maintaining their erections even prior to ejaculation. Since they feel consciously or subconsciously pressured during intercourse to ejaculate prior to losing their erections, they can sometimes get into the habit of having premature ejaculation.
But let’s assume that the erectile dysfunction preceded the premature ejaculation. Usually, then we’d deal with the erectile dysfunction as the primary issue. Often, when these men can achieve successful and long-lasting erections, they will not ejaculate as quickly. If after treatment for erectile dysfunction the premature ejaculation remains a problem, we would look at that separately.
You and your doctor may discuss other subjects depending on his thoughts on diagnosis. These include:
After ejaculation, how long does it take you to have a second erection and reach an orgasm?
This information will be useful in determining treatment options. Some men have long-standing premature ejaculation, but their habit has been to ejaculate quickly (either through masturbation or with their partner) for the first ejaculation and then to have more leisurely intercourse because they last longer the second time. Many of these men come to the physician when they get older or have other medical problems and lose the ability to get a rigid second erection in the same lovemaking session. At this point, the premature ejaculation interferes significantly with their lovemaking.
How often do you ejaculate?
This can be either through masturbation or with a partner. Many men who develop premature ejaculation do not have satisfying sexual experiences. Because of this, they become somewhat avoidant of sexual situations even in the context of a relationship or marriage and have decreased frequency of intercourse and ejaculation. With decreased frequency and longer time periods between ejaculations, many men will ejaculate more quickly. Premature ejaculation can then become a vicious cycle. One of the ways of breaking the cycle is to encourage the man to ejaculate at some point prior to intercourse so that he will then last longer during intercourse.
How has the premature ejaculation affected your relationship?
Often, premature ejaculation is a chronic problem. For many couples, this has caused significant disturbance in their sexual relationship. Many partners harbor significant resentment, especially if this is a problem that the man has refused to address for a number of years. Usually, a partner is very grateful that the man has sought treatment because it shows that he understands there is a problem and would like to satisfy his partner more completely.
Have you had prior treatments?
If you have been placed on medication, it is important to know which medication and the dosage. If you have done any behavior modification, it is important to let the physician know this as well.
Evaluation and Diagnosis with a Physical Exam
The most important part of the evaluation is the history. It is worthwhile to think about the answers to these questions prior to your appointment:
- Is the premature ejaculation lifelong, or acquired?
- Is it in all situations, or just some?
- How long do you last, after penetration, and before ejaculation? Do you ejaculate before penetration?
- How much does this bother you, and/or your partner?
- What is your refractory time, in terms of from the time you ejaculate until you can get another erection and/or ejaculate again?
- What makes it better?
- What seems to make it worse?
- Do you have erection issues?
- Do you have prostate issues?
- Do you have symptoms of hormonal issues?
Physical Exam
As part of your evaluation for premature ejaculation you will have a focused physical exam.
We will examine your penis and testes and if appropriate consider a prostate exam.
We will also do a simple painless interesting test called biothesiometry. This measures your sensitivity to vibration, both on your fingers and penis. Men with premature ejaculation have been found to have more sensitive penises. We have sometimes been astounded at how sensitive some men can be to vibration.
Studies have shown that not only are many men with PE hypersensitive, their ejaculation reflex is very quick as well. This has been measured, in studies, by how fast a signal given on the penis is registered up in the brain, and then transmitted back into the genitals. This is not something you can consciously change–it shows that it is the way you are built.
IN A PATIENT'S OWN WORDS
I had been suffering from PE for many years and had become so frustrated and depressed about sex. Finally, I decided I needed to seek treatment. I was referred to Doctor Werner by my doctor and after my first appointment, I was prescribed a regimen of medication and cream.
The treatment plan worked! Doctor Werner and the Maze team have helped me gain back my confidence and reduce my anxiety. They’ve changed my life. I would highly recommend Maze to anyone experiencing PE.
- G, 37 -
Last updated: March 2023